 |
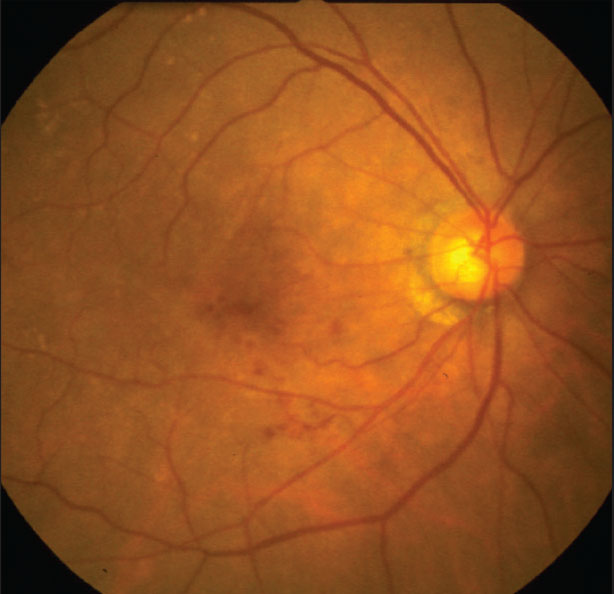
Preventive measures and prompt intervention are essential for combating the potentially vision-threatening complications of diabetic retinopathy. In the early stages of this disease, retinal damage manifests without obvious symptoms, becoming apparent later as vision starts to deteriorate. Fortunately, advances in imaging technologies like OCT and OCTA enable clinicians to detect and monitor subtle early changes, such as those in central macular thickness and the foveal avascular zone area. In a recent Clinical Ophthalmology paper, Chinese researchers identified and linked potential systemic risk factors to early structural changes for improved intervention.1
In the cross-sectional study, 60 healthy controls, 60 patients with no DR and 60 patients with mild NPDR underwent comprehensive eye exams with OCT and OCTA imaging. The researchers observed significant differences in CMT and FAZ area in the eyes of diabetic patients compared to those of the healthy control group; and between NPDR eyes and eyes without diabetic retinopathy.
The analysis revealed that central macular thickness had a positive correlation with a number of systemic metabolic markers, including duration of diabetes, BMI, total cholesterol, triglyceride, and systolic and diastolic blood pressure. FAZ area was positively correlated with duration of diabetes and BMI.
In their paper, researchers recommend that in clinical practice, diabetic patients—particularly those with longer disease duration, abnormal lipid levels, high blood pressure and obesity—“should undergo enhanced macular examination and monitoring to detect signs of retinal lesions early and promptly implement comprehensive treatment measures, including blood glucose, lipid and blood pressure control, and weight reduction, to slow disease progression.”
REFERENCE
1. Wei W, Wang W, Qiu Q. Central macular thickness and foveal avascular zone are indicators of early diabetic retinopathy. Clin Ophthalmology 2025;19:3505-3514.
Study Finds Metformin is Ineffective Against AMD
Prescription drugs are carefully formulated to treat specific diseases and conditions; however, unanticipated effects (both good and bad) are often identified “in the wild” and some drugs then undergo further testing to explore other indications of use. Several diabetes medications have demonstrated positive as well as negative effects in recent years and have proven a fruitful area for research. In a new JAMA Ophthalmology paper, researchers observed the use of anti-diabetic drug metformin and its potential effects to protect against the development and progression of age-related macular degeneration.1
Using the TriNetX database, researchers gathered electronic health record information from 70 institutions to answer whether or not metformin is associated with the development and progression of AMD.
Subjects who met the inclusion criteria were divided into two cohorts: one with and one without a diagnosis of AMD. AMD was identified using ICD codes in the records.
Observations revealed no significant association between metformin and the development and progression of AMD.
The cohort with no history of AMD comprised 297,008 individuals prescribed metformin and 1,269,644 individuals without a history of metformin use. The second cohort, this time of AMD patients, was much smaller in population, enlisting 12,843 individuals prescribed metformin and 77,279 individuals without a history of use. When the researchers employed propensity score matching, they discovered that the risk of developing AMD was comparable between participants prescribed and those without a prescription of metformin (relative risk: 0.90). Furthermore, similar results for the risk of progression to neovascular or geographic atrophy were observed between the two groups.
“Further studies and prospective analyses are necessary to better evaluate whether dosage and longevity of metformin use may influence AMD development or progression,” conclude the authors of the paper.
There were multiple limitations that led to this notion. For instance, metformin is typically prescribed to type 2 diabetes patients, and other prescription drugs were not taken into account for this study. Additionally, the assessment of metformin use was limited by the data, and adherence to the drug couldn’t be examined. Other data points such as quantity, frequency and longevity of the prescriptions weren’t available either. Lastly, EHR data isn’t perfect, and the ICD could have been misclassified, leading to limited results.
An invited commentary also published in JAMA Ophthalmology noted additional shortcomings of this study.2 It addressed the fact that EHR data can present significant challenges when analyzing the potential advantages and disadvantages of metformin. When selecting participating data for their study, researchers excluded individuals without ICD codes for AMD. The commentary authors stated that this doesn't definitively entail the absence of this ocular condition, since subjects may be experiencing AMD without a diagnosis.
Another flaw pointed out by the commentators was the unavoidable inclusion of the differential measurements of outcomes. They explain that patients prescribed metformin typically undergo regular screening for diabetic retinopathy, while others most likely don’t receive such care and observation; therefore, conditions such as AMD can go overlooked.
One suggestion for future researchers is to conduct studies with a target trial emulation framework. While this model uses observational data similar to the propensity score matching model seen in the aforementioned study, target trial emulation’s design takes the data and mimics a randomized clinical trial. This, the commentators believe, could help mitigate biases seen in traditional analyses.
The commentary did highlight some positive outcomes from this study. It recognized the study authors’ “careful interpretation of findings and for clearly acknowledging the many limitations of their analysis.” Outcomes were noted as a valuable reminder of what can be expected when conducting a study using data to explore how drugs can be repurposed for other opportunities.
“Until high-quality causal evidence is available, the totality of the currently available evidence does not support the consideration of clinicians to prescribe metformin for the sole purpose of preventing AMD or slowing its progression,” the commentary authors conclude.
REFERENCES
1. Jindal DA, Hanna J, Shaia JK, et al. Metformin and the development of age-related macular degeneration. JAMA Ophthalmol. September 18, 2025. [Epub ahead of print].
2. Liu SH, Mandava N, Li T. Metformin and age-related macular degeneration—No causal evidence yet. JAMA Ophthalmol. September 18, 2025. [Epub ahead of print].
Anti-thrombotics and Hemorrhage Risk in Wet AMD
Korean investigators examined the association between anticoagulant or antiplatelet use and clinically important intraocular hemorrhage requiring vitrectomy in patients with wet AMD.
The nationwide, population-based, retrospective cohort study analyzed 149,620 patients with exudative AMD older than 40.1
The main study outcome was clinically important intraocular hemorrhage requiring vitrectomy. All analyses were adjusted for demographics and comorbidities.
A total of 94,449 patients (mean [SD] age, 71.8 [9.8] years; 55,677 [59 percent] male) were included in the cohort study, and 8,110 patients (mean [SD] age, 70.2 [9.6] years; 5,090 [62.8 percent] male) were included in the case-control study.
In the Cox proportional hazards regression analysis, anticoagulant or antiplatelet exposure was associated with a higher risk of intraocular hemorrhage requiring vitrectomy. The incidence probability of intraocular hemorrhage requiring vitrectomy was higher in the exposure group than the nonexposure group.
In the logistic analysis, the use of anticoagulants (adjusted odds ratio [aOR], 1.88; CI, 1.45 to 2.44) or antiplatelets (aOR, 1.37; CI, 1.19 to 1.57) was associated with intraocular hemorrhage requiring vitrectomy.
The combined use of anticoagulants and antiplatelets showed the highest aOR.
Higher medication adherence was also associated with a higher aOR of intraocular hemorrhage.
Investigators found, in this nationwide cohort study of patients with wet AMD, antithrombotic medications were associated with a higher risk of intraocular hemorrhage requiring vitrectomy. They note that the results suggest the need for proactive communication and tailored monitoring strategies. RS
REFERENCE
1. Kim MS, Nam S, Lee J, et al. Antithrombotic medications and intraocular hemorrhage risk in exudative age-related macular degeneration. JAMA Netw Open. Sep 2, 2025. [Epub ahead of print].