|
Bios |
The concept of lamellar macular hole was first reported by Gass et al. in 1976.1 Subsequently, OCT illustrated that a thick proliferative tissue often accompanies LMH on the macula, which was named lamellar hole-associated epiretinal proliferation. In eyes with LMH, removing LHEP doesn’t necessarily result in improved postoperative vision and a full-thickness macular hole is sometimes developed postoperatively.
Dr. Fumio Shiraga reported that embedding LHEP into the hole achieved favorable outcomes.2 In the original method, LHEP is peeled from the ILM using microforceps and embedded into the hole while keeping it attached to the edge of the hole. This technique requires precise handling of the microforceps. If the LHEP is gripped too deeply, it may damage the underlying sensory retina or ILM, potentially causing scotomas. Additionally, LHEP is sticky and may adhere strongly to the microforceps’ tips, leading to unintentional removal from the hole’s edge.
Here, we describe a new method we’ve developed that uses a backflush needle instead of the forceps to achieve successful LHEP embedding.3
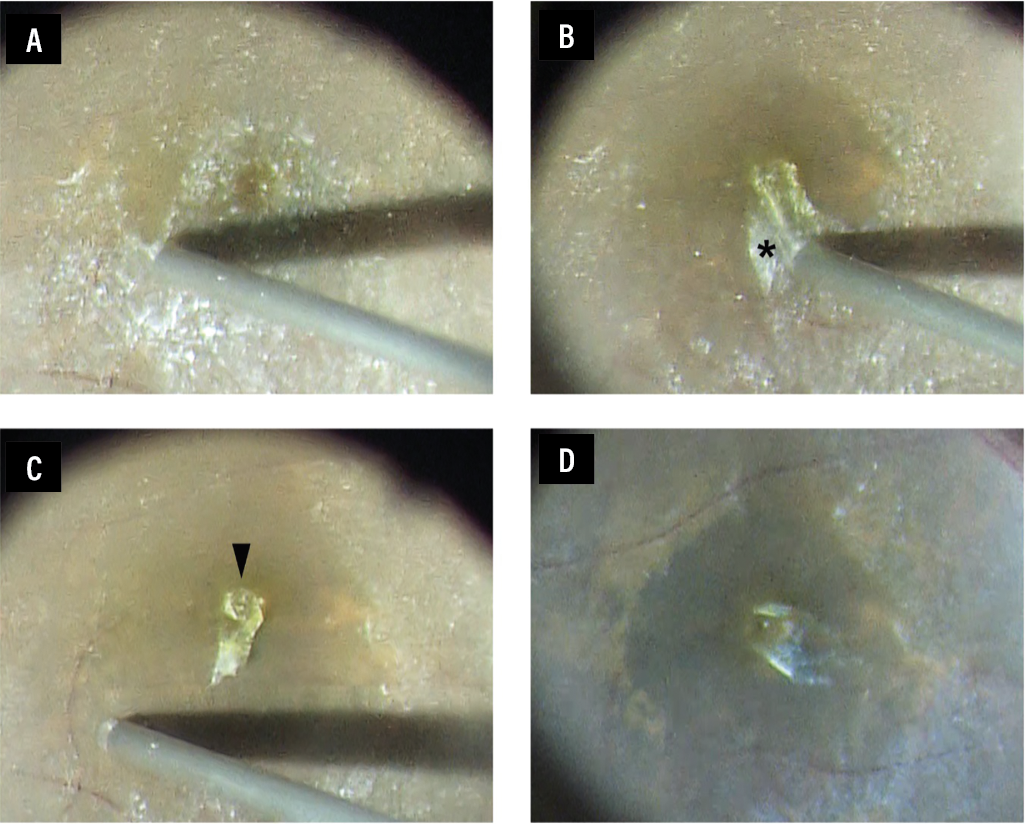 |
| Figure 1. (A) The membrane is visualized with triamcinolone acetonide. (B) The thin preretinal membrane, a non-yellowish tissue (asterisk), is peeled centripetally using a 25-gauge disposable Shiraga backflush instrument with an extendible brush tip (D.O.R.C./Zeiss) and passive aspiration. (C) The thin preretinal membrane is selectively removed by passive aspiration, but the LHEP, which appeared as a yellowish tissue (arrowhead), remains adjacent to the hole. (D) Staining of the ILM with BBG reveals that the entire ILM is stained, suggesting that the ILM in the area of the thin preretinal membrane peeling remains intact. |
Surgical technique
After a core vitrectomy, we use triamcinolone acetonide to visualize a thin preretinal membrane on the macula (Figure 1A), which we peeled using a silicone-tipped backflush needle with “passive” aspiration (the irrigation pressure was set to 20 mmHg). We then gently peel the thin preretinal membrane centripetally and remove it, leaving the LHEP adjacent to the hole (Figure 1 B, C). Although we selectively remove the thin preretinal membrane by passive aspiration, the LHEP remains on the edge of the hole because of its strong adhesion.
We then peel the ILM using Brilliant blue G. The entire ILM is stained without any damage (Figure 1D), suggesting that the ILM in the area of the thin preretinal membrane peeling remains intact. We then embed the remaining LHEP into the hole, followed by a fluid-air exchange to conclude the surgery. The technique has three advantages:
1. It simplifies the peeling process, eliminating the need for advanced microforceps skills.
2. Passive aspiration selectively removes the thin preretinal membrane while preserving the LHEP at the LMH edge.
3. The technique minimizes retinal damage, as shown by uniform internal limiting membrane staining after membrane peeling.
Important considerations
To avoid excessive aspiration near the macula, we’ve found it’s safer to turn off IOP control in the Constellation system (Alcon), which is the device we use. Starting the peeling process about two disc diameters away from the macula and using BBG or triamcinolone for better visualization can help, though the method may not work for LMH cases with thick ERM.
Final thoughts
In summary, the LHEP embedding technique using a backflush needle offers a simpler, safer and more controlled alternative to traditional microforceps-based methods. By relying on passive aspiration to selectively peel the thin preretinal membrane while preserving and embedding the LHEP, this approach maintains ILM integrity and enhances reproducibility among surgeons. RS
References
1. Gass JDM. Lamellar macular hole: A complication of cystoid macular edema after cataract extraction. Archives of Ophthalmology 1976;94:793-800.
2. Shiraga F, Takasu I, Fukuda K, et al. Modified vitreous surgery for symptomatic lamellar macular hole with epiretinal membrane containing macular pigment. Retina 2013;33:1263-1269.
3. Fukushima M, Hayashi A, Kusaka S, et al. Use of a backflush needle with a silicone tip cannula to embed lamellar hole-associated epiretinal proliferation. Retina 2023;43:12:2204-2207.