 |
|
Bios Ms. Lam is an undergraduate student at Columbia University. Dr. Hu is a uveitis fellow at Massachusetts Eye and Ear Infirmary. Dr. Mylvaganam is a partner at New England Retina Consultants in Springfield, Mass. |
A 59-year-old Asian American woman was referred for bilateral anterior uveitis. She reported one week of eye redness and photophobia. Evaluation with her optometrist showed 20/20 VA OU, 1+ WBCs in the anterior chamber and fine corneal endothelial keratic precipitates OU. The patient was started on topical prednisolone q.i.d. and cyclogyl b.i.d.
Our first exam
At our office, the patient’s symptoms persisted. Past medical history was significant for hypertension. Her review of systems was significant for mild neck stiffness and mild cold symptoms. There was no family history of uveitis or other autoimmune diseases. Her vision was 20/30 OD and 20/25 OS. IOP was 12 mmHg OU. Slit lamp exam displayed 2+ WBCs OU. Fundus exam showed posterior vitreous detachments but no vitritis OU. There was a moderate epiretinal membrane OS.
The patient’s prednisolone was increased to six times a day. She was instructed to see her primary care doctor and the following medical work-up was ordered: CBC; complete metabolic panel; Lyme; HLA-B27; ACE; CRP; ANA; toxoplamosis IgG and IgM; QuantiFERON-TB; CXR, HIV; VZV; HSV 1&2; RPR; ANCA; beta 2 microglobulin; urinalysis; anti-PR3; and anti-MPO ANCA—all of which were normal. However, the following tests were positive: ESR (32); CRP (18); and ANA (1:160 speckled pattern).
Follow-up exam
On follow-up two weeks later, the patient was increasingly symptomatic with worsening floaters and photophobia OU. She had also developed worsening cold symptoms, chest congestion and headaches. She noticed that the cartilage in her nose and ears was tender.
The patient’s vision was 20/40 OU. Her anterior chamber inflammation was stable but she had developed 2+ vitritis OD and 1+ vitritis OS. A new cotton wool spot was noted in her macula OD.
 |
|
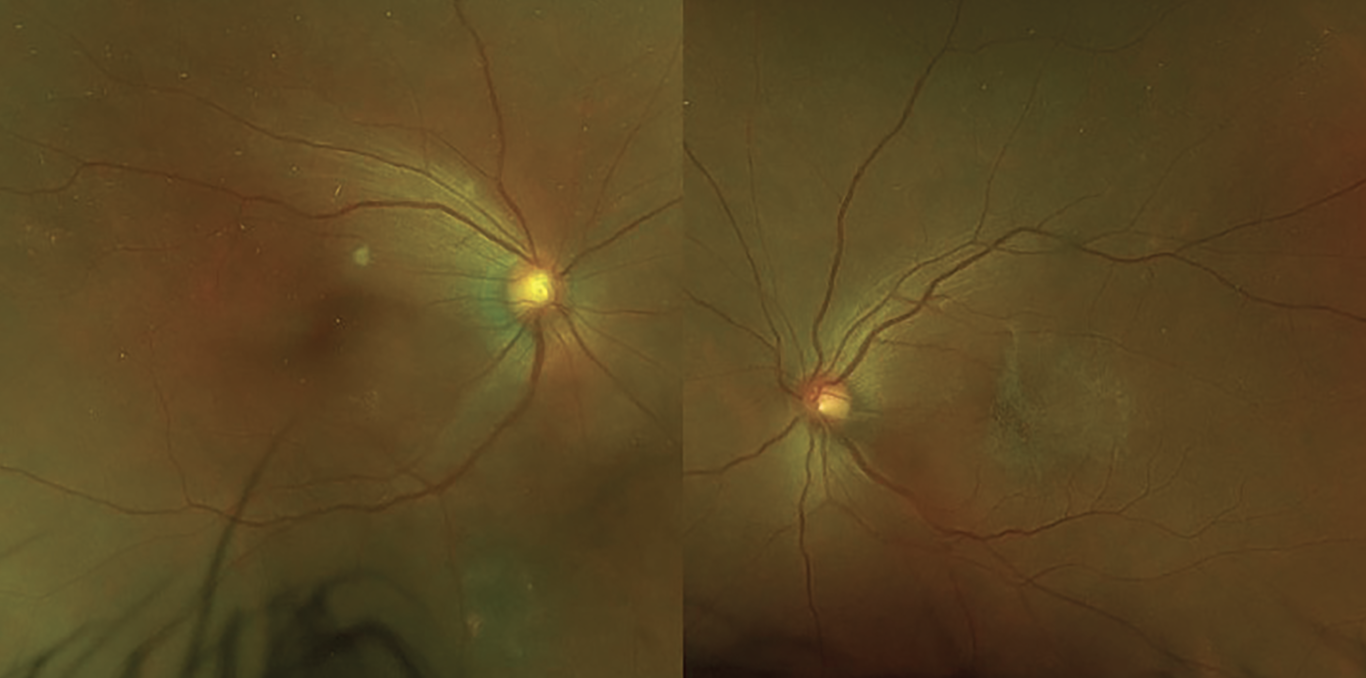
Figure 1. Pseudocolor fundus photos displaying a cotton wool spot in the right eye and epiretinal membrane in the left. |
Diagnosis and management
The patient’s ear and nose tenderness, accompanied by worsening ocular inflammation prompted consideration of relapsing polychondritis as a diagnosis. The patient was referred to a tertiary medical center for a uveitis consultation. Fluorescein angiography displayed significant peripheral vascular leakage and dilation of capillaries in all quadrants OU. There was cystoid macular edema in the left eye, confirmed by both by OCT and FA. She was treated with one dose of 1g IV solumedrol followed by 60 mg oral prednisone daily. Her visual symptoms were stable, but she had developed joint pain in her elbows.
The patient was seen for follow-up two weeks later. Her vision was 20/40 OD and 20/60 OS. Her intraocular inflammation had improved to 1+ and trace AC cell OD and OS respectively. Her nose and ear tenderness had resolved. The patient was tapered off oral prednisone. One month following initiation of systemic steroid treatment, her BCVA improved to 20/25 OU and examination showed resolved AC and vitreous inflammation.
 |
|
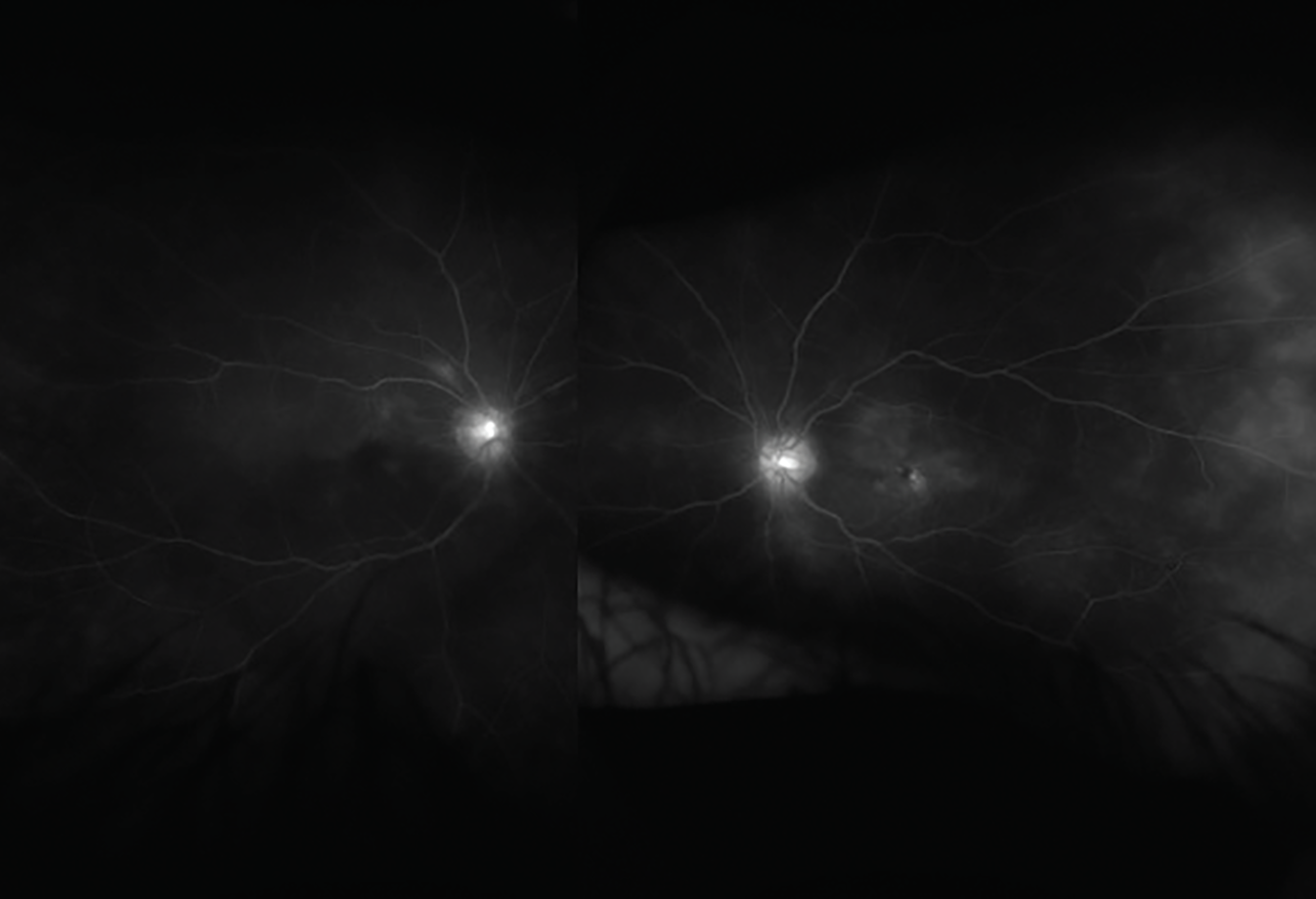
Figure 2. Fluorescein angiogram showing extensive macular and peripheral vascular leakage in the right and left eyes. |
Discussion
Relapsing polychondritis is a rare autoimmune condition that typically presents with cartilaginous inflammation of the auricular, nasal or tracheal cartilage. Its etiology is unknown. It has no predilection for either sex, and occurs in all races.1 The propensity for cartilaginous symptomatology implies an immune reaction against proteoglycan, the main component of cartilaginous tissue.1 Ear involvement is seen in 90 percent of cases. Ocular manifestations such as episcleritis, scleritis and uveitis can be seen in 20 to 60 percent of cases. Inflammation of the cartilaginous rings of the trachea can be life-threatening if tracheobronchomalacia—collapse of the airway—occurs. 1
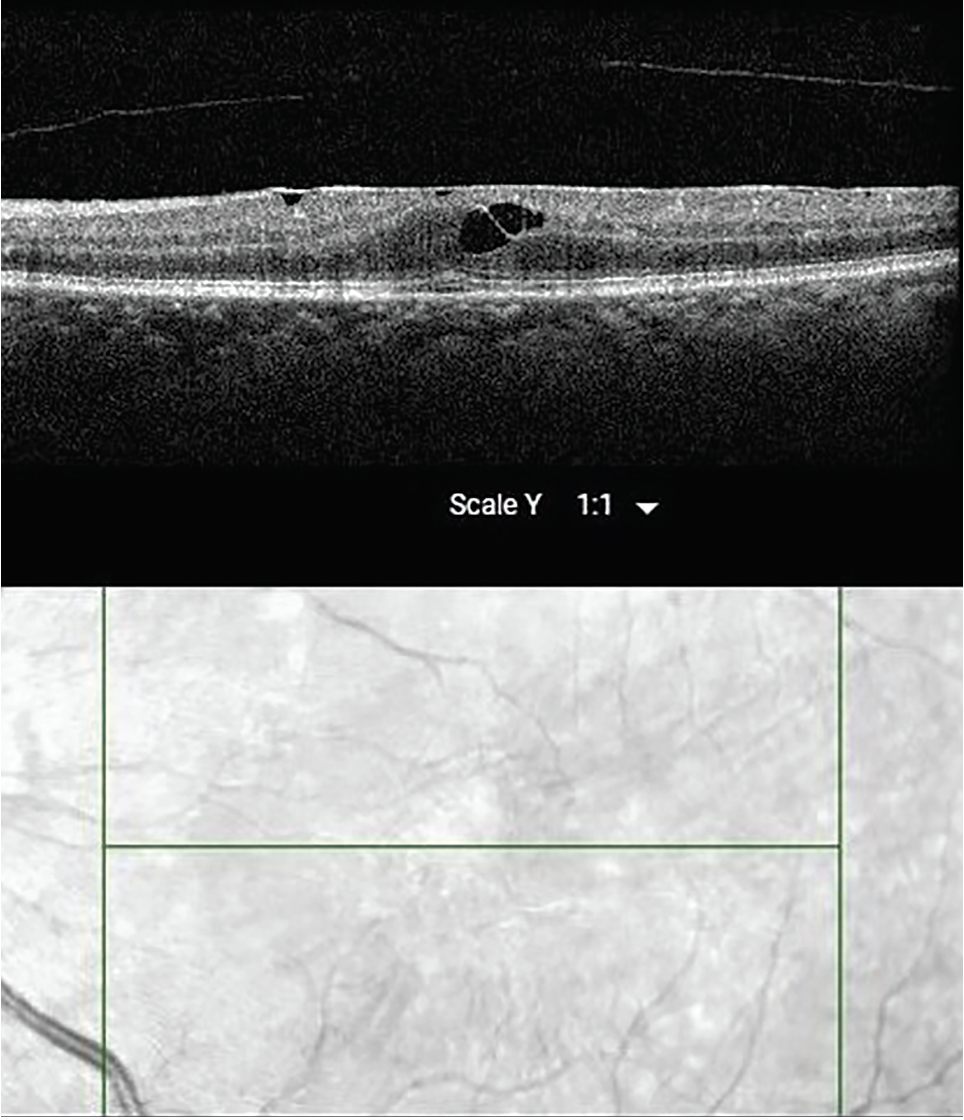 |
| Figure 3. OCT of the left eye showing epiretinal membrane and cystoid macular edema. |
Relapsing polychondritis is primarily a clinical diagnosis. Although biopsy of auricular cartilage can be considered, it’s rarely performed. More commonly, the diagnosis is made by having three of the following six criteria:1
- recurrent chondritis of both auricles;
- non-erosive inflammatory polyarthritis;
- chondritis of nasal cartilage;
- inflammation of ocular structures;
- chondritis of the respiratory tract; and/or
- cochlear or vestibular damage.
Treatment is determined by the severity of clinical symptoms and there’s no standardized treatment regimen. Non-steroidal anti-inflammatory agents and corticosteroid treatment are commonly employed for mild cases.1 In severe cases with airway involvement, immunosuppressive treatment with cyclophosphamide, methotrexate or cyclosporine may be considered. Biologic alternatives include a TNF-alpha inhibitors as well as rituximab.1
Relapsing polychondritis is often a diagnosis of exclusion. The differential diagnosis includes: tuberculosis, syphilis, ANCA-associated vasculitis, and polyarteritis nodosa.1 Patients with relapsing polychondritis may have recurrent episodes and very severe disease—respiratory failure is the most perilous sequelae. However, more commonly the clinical course is mild and successfully medically managed.
This case illustrates the importance of obtaining a complete review of systems. Here, the patient’s complaint of nose and ear cartilage tenderness raised suspicion of relapsing polychondritis which was then treated promptly and aggressively. RS
Reference
1. Rose T, Schneider U, Bertolo M, et al. Observational study and brief analysis of diagnostic criteria in relapsing polychondritis. Rheumatology International 2018;38:2095-2101.